New potential treatments for low libido and difficulties with arousal in women

These products were developed based on the biology of sexual excitation and inhibition in women
These treatments were developed by Dr. Adriaan Tuiten and his team in the Netherlands, with the understanding that there are multiple biological pathways of low sexual desire or arousal in women. According to their research, some women’s brains are less responsive to sexual cues, and some become inhibited in response to sexual stimulation.
The drug treatments described in this study both contain testosterone to affect sexual motivation and/or desire, paired with a second medication to address one of the other causes mentioned above.
What are the treatments being tested?
There were two treatments tested in the study:
Who is it for?
Women with low sensitivity to sexual stimuli
Women with high sexual inhibition
What is in it?
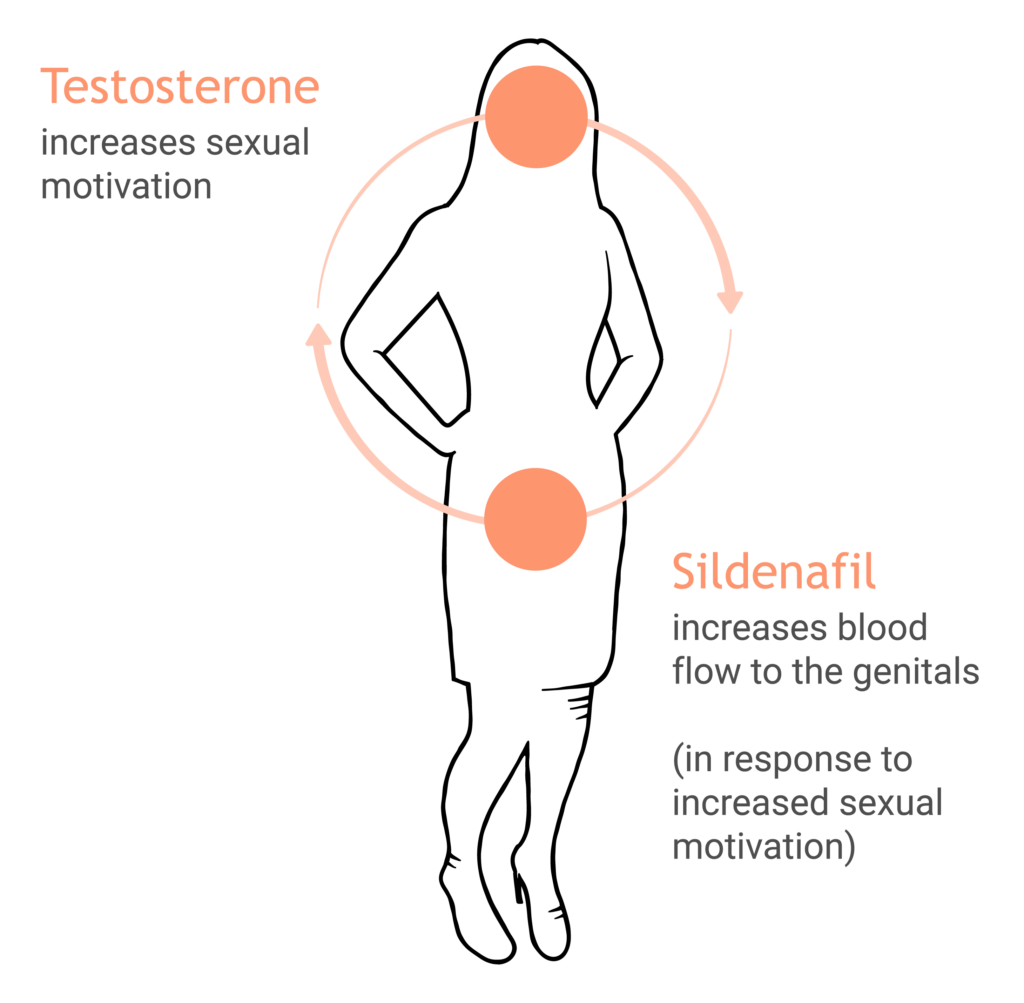
Testosterone (T) and sildenafil (S)
Testosterone (T) and buspirone (B)
What is in it?
Testosterone (T) and sildenafil (S)
Who is it for?
Women with low sensitivity to sexual stimuli
How does it work?
What is in it?
Testosterone (T) and buspirone (B)
Who is it for?
Women with high sexual inhibition
How does it work?
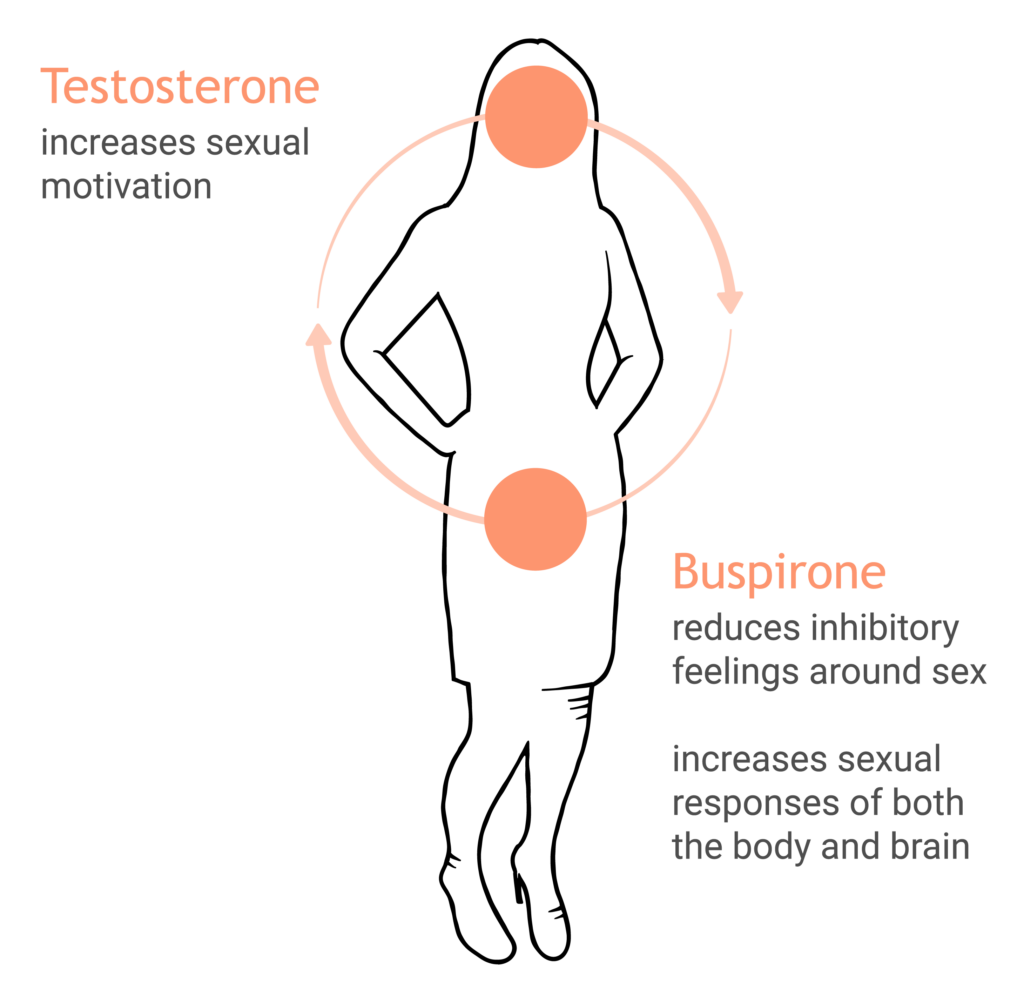
Both treatments are tablets with testosterone on the outside and the second medication (S or B) on the inside. First the testosterone is absorbed into the bloodstream, which leads to an increase in sexual motivation (increased interest in sexual activity) three to six hours later. This signals the body to increase vaginal arousal.
This study was done to determine whether and how well these treatments could work.
Who participated?
Studies were conducted with American women between 21 and 70 years old who had been diagnosed with low sexual desire and/or arousal with distress by a medical professional.
Participants were categorized as being in either the low sensitivity or the high inhibition group through a calculation of genetic, hormonal, and psychological variables. Within each patient group, the women were randomized to receive either a placebo, or a single or combination medication appropriate for their categorization (T, S, or T+S for the low sensitivity group; T, B, or T+B for the high inhibition group).
Outcomes were measured by asking participants to record the number of sexually satisfying events (SSEs), provide subjective sexual satisfaction of each event, and the number of orgasms over the course of the study.
Positive results
For both groups of participants taking combination treatments (T+S and T+B), the women reported significantly more sexual satisfaction and orgasms than those who took the placebo, and more than those taking only one of the two components on their own (only T or only S, for example).
Of the participants identified as having low sensitivity to sexual cues (taking the T+S treatment), they reported having more sexually satisfying events than placebo or a single treatment (an increase of at least 1-2 events during the study period was considered clinically relevant).
Conclusions
Both treatments were shown to be effective for each category of participants. This shows that having an understanding of the biological causes of low sexual desire or arousal are important in developing targeted treatments for women.
Reference article:
Tuiten A. et al. (2008) Efficacy and safety of on-demand use of 2 treatments designed for different etiologies of female sexual interest/arousal disorder: 3 randomized clinical trials. J Sex Med. 15(2):201-216.